

Introduction
Clear cell hidradenoma is a skin adnexal tumor originating from eccrine glands that was first referred to as myoepithelioma,1) and subsequently as clear cell hidradenoma, eccrine acrospiroma, nodular hidradenoma, and solid cystic hidradenoma.2-4) Clear cell hidradenoma most commonly occurs on the head and neck, and may present as a single papule, nodule, or mass. The lesions are most commonly red, but may also be brown or skin-colored. Clear cell hidradenoma is usually asymptomatic, but may be accompanied by bleeding, pain, or discharge. Clinically, clear cell hidradenoma is characterized by a single intradermal nodule that is present for a prolonged duration before sudden growth or recurrence after surgical removal. Malignant clear cell hidradenoma tends to metastasize to the regional lymph nodes, lung, liver, and pericardium.5,6) This type of tumor is very difficult to diagnose clinically, and the histological findings of clear cell hidradenoma vary considerably. Therefore, these tumors pose a major diagnostic challenge.7) The treatment for clear cell hidradenoma is surgical resection. We report a case of clear cell hidradenoma of the posterior neck in a 70-year-old woman.
Case Report
This case occurred in a 70-year-old woman who had a history of treatment for syphilis in 2015, was taking 0.1 mg of Synthroid to treat hypothyroidism, and had undergone stent implantation in 2018 due to coronary heart disease. She was taking 100 mg of aspirin and 12.5 mg of carvedilol (an antilipidemic agent and vasodilator). She noted a tiny mass on her left neck 1 year earlier. She thought the mass was acne and therefore picked at it by hand several times. There was no pain or tenderness, but despite the patientŌĆÖs attempts to remove the mass by hand, it gradually grew to the size of a nipple. One morning, she woke up and found a bloody spot on her pillow, which prompted to her to seek care at a local hospital in October 2018. At that time, the size of the lesion was 3.0 ├Ś 1.5 ├Ś 1.5 cm. After an excisional biopsy, clear cell hidradenoma was diagnosed based on a histological examination. However, the tumor recurred and she presented to our outpatient clinic in January 2019.
Upon a physical examination, a single 1.5 ├Ś 0.7 cm mass was seen on the left posterior neck area with skin color changes (Fig. 1). The mass was mildly firm, non-fluctuant, non-tender, and non-movable. No abnormality other than the left posterior neck lesion was noted. Some erythema was present, but no tenderness. No enlargement of the peripheral lymph nodes or any other abnormal findings were observed in the general and neurological examinations. No relevant abnormalities were found on positron emission tomography-computed tomography (PET-CT), abdominal computed tomography (CT), or chest CT.
Fig.┬Ā1
Preoperative condition of the patient. A 70-year-old woman presented to our outpatient clinic. Upon physical examination, a single 1.5 ├Ś 0.7 cm mass was seen on the left posterior neck area with skin color changes. The mass was mildly firm, non-fluctuant, non-tender, and not movable. No abnormality other than the left posterior neck lesion was noted. Some erythema was present, but no tenderness. No enlargement of the peripheral lymph nodes or any other abnormal findings were observed in the general and neurological examinations.

Excisional biopsy was performed under local anesthesia. Because it was a recurrent lesion, wide excision was performed with a 1-cm margin from the main nodule (Fig. 2A). This widely and circularly excised main mass were sent to the pathology department, and a frozen -section biopsy test was performed on this tissue. The intraoperative findings were a cystic mass with clear border containing a solid nodule. Frozen-section biopsy showed that the specimen containing main mass has a sufficient tumor cell free zone of 0.5 cm or more medially from the resection margin. On the other hand, the main specimen had 0.1 cm of tumor cell free zone on its base (deep margin). Therefore, it was decided not to do further circumferential excision under clinical consideration, but additional excision of the fascia of the sternocleidomastoid muscle was performed in the deeper direction. This second tissue specimen was sent to pathology department, and the absence of tumor cells was confirmed by secondary frozen-section biopsy examination. A bilobed flap was elevated to cover the 3.5 ├Ś 2.7 cm defect, with careful hemostasis (Fig. 2B). However, a hematoma formed on the evening of the day of surgery. We returned the flap to its preoperative position after evacuating the hematoma, waited for 3 days for the site to stabilize, and then completed the transfer of the delayed bilobed flap (Fig. 2B). No prophylactic lymph node dissection, radiotherapy, or chemotherapy was performed.
Fig.┬Ā2
Wide excision and bilobed flap design. (A) Wide excision was performed with a 1-cm margin and frozen-section biopsy was conducted. The intraoperative findings were a cystic mass with a clear border containing a solid nodule. (B) To cover the 3.5 ├Ś 2.7 cm defect, a bilobed flap was performed with careful hemostasis to prevent bleeding.

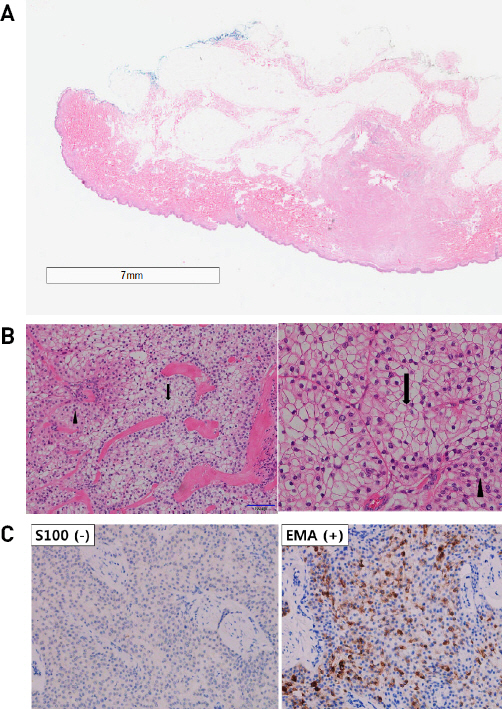
As a result of the permanent histopathologic examination, the main nudular mass was a recurrent clear cell hidradenoma with negative resection margins. On a histological examination, clear cell hidradenoma may be associated with the epidermis or several large lobules extending from the dermis to the subcutaneous fat layer. The tumor contains two types of cells (clear and cuboidal), and cysts, ducts, or solid areas are observed within the lobules (Fig. 3A). In this case, both types of cells were observed (Fig. 3B). And immunohistochemical analyses showed negative findings for S100 protein and carcinoembryonic antigen (CEA), and focal positivity for epithelial membrane antigen (EMA). Therefore, the tumor was relatively unlikely to be malignant (Fig. 3C). EMA can be expressed in the secretory portion of benign tumors, while it shows an inconsistent pattern of expression in malignancies.8)
Fig.┬Ā3
Histological examination. (A) The tumor was composed of clear and cuboidal cells, and cysts, ducts, and solid areas were observed within the lobules (H&E stain, x 12.5). (B) Clear cells (arrow) and cuboidal cells (arrow head) were distinguished. (H&E stain, right figure : x 200 / left figure : x 400). (C) Immunohistochemistry showed negative findings for S100 protein and carcinoembryonic antigen (CEA), as well as focal positivity for epithelial membrane antigen (EMA), indicating that the tumor was unlikely to be malignant.
Discussion
Clear cell hidradenoma more commonly affects individuals above the age of 50 than their younger counterparts, and it shows no predilection according to sex or race.9) It usually occurs on the head and neck, and it presents as intradermal nodules ranging in size from 0.5 to 2.0 cm.9) The risk of local recurrence after surgical resection exceeds 50%. Recurrent clear cell hidradenomas are activated by surgical stimulation, increasing the risk of metastasis.10) When diagnosing clear cell hidradenoma, it is important to determine the likelihood of malignancy, as 6-19% are malignant.11) Malignant clear cell hidradenoma shows a pattern of long-lasting asymptomatic enlargement, followed by sudden growth caused by an external stimulus such as trauma, electrocautery, or incomplete resection.12) To treat recurrent clear cell hidradenoma appropriately, it is important to obtain a clear impression of the lesion based on histological and imaging examinations.13) Clear cell hidradenoma is characterized by a well-defined margin in the subcutaneous fat layer with or without involvement of the dermal layer.14) The histological findings of malignant clear cell hidradenoma include large, unclear margins, and invasive tumors form lobe structures containing intralobar clear cells and epidermoid cells.14) Immunohistochemical staining for S100 protein, CEA, and EMA is also helpful for the diagnosis.15)
In this case, the tumor grew in response to manual stimulation and recurred after incomplete resection. Based on its histological findings, the tumor was considered to be benign, and complete surgical resection was performed. The primary treatment for recurrent clear cell hidradenoma is total resection, so it is important to ensure a clear resection margin. However, no consensus exists in the literature regarding the appropriate resection margin, and reported resection margins range widely, from several millimeters with Mohs micrographic surgery to 2 cm with wide excision.16-18) Will et al. stated that adequate primary local excision is very important and proposed that Mohs micrographic surgery should be performed in recurrent cases.16) In 2006, Liapakis et al. argued for wide excision, with a margin of at least 2 cm, in cases of malignancy.17) More recently, Park et al. suggested wide excision of the free margin to reduce recurrence as the first-line treatment even if no malignant findings are observed.18)
In this case of recurrent clear cell hidradenoma, we reconstructed the defect with a bilobed flap after 1-cm wide excision. No local recurrence was noted during one and a half years of follow-up (Fig. 4). In patients with recurrent clear cell hidradenoma, is also important to consider post-resection reconstructive surgery and its cosmetic results. Since even benign clear cell hidradenoma poses a high risk of local recurrence, it is recommended to achieve a tumor-free plane, as confirmed with frozen-section biopsy, after excision with a 1-cm margin as the first line of treatment, rather than performing a minimally invasive resection or a wide excision (Ōēź2 cm).





