

서론
원발성 갑상선 편평상피세포암은 전체 갑상선 암 중에서 1% 정도로 매우 드물게 발생하는 질환으로,1) 2012년 기준으로 세계적으로 84례가 보고되었으며2) 국내에서는 13례가 보고되었다.3) 갑상선에서 발생하는 원발성 편평상피세포암은 모든 연령층에서 발생 가능하지만, 주로 50, 60대에서 발생한다고 보고된 바 있으며 인접한 장기를 침범한 형태로 진단되는 경우가 많고, 임상적 경과 및 예후가 매우 불량하다.4,5) 수술 및 방사선 치료 후에도 국소 재발이 빈번하여 평균 생존기간이 1년 미만으로 역형성암종(anaplastic carcinoma)과 마찬가지로 공격적인 임상적 경과를 보인다.4) 발생기원에 대하여 여러 가설이 존재하나, 최근에는 갑상선 여포세포가 이차적으로 편평상피화생을 일으켜 암성 변화를 유발한다는 설이 지배적이다.6)
저자들은 원발성 갑상선 악성 종양의 극히 드문 형태인 편평상피세포암 1예를 경험하였고 국내 문헌에는 이에 대한 보고가 많지 않아 문헌고찰과 함께 보고하는 바이다.
증례
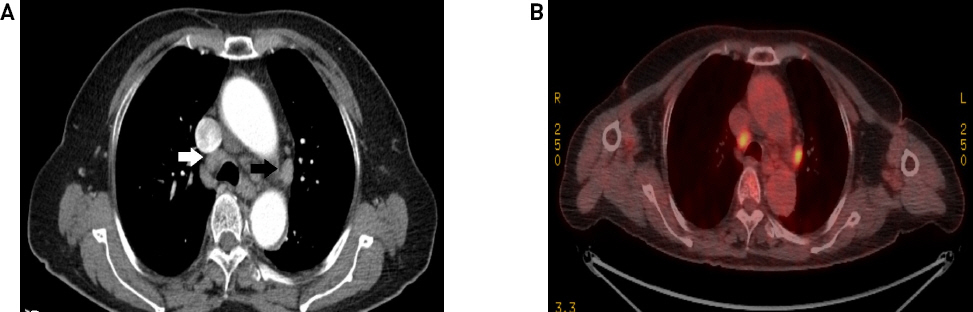
79세 여자 환자가 내원 10일 전부터 크기가 증가하며 통증을 동반하는 전경부 종괴를 주소로 내원하였다. 환자는 고혈압, 당뇨, 뇌경색 과거력으로 약물 복용 중이었으며, 6개월전 양안 백내장 수술을 받은 병력이 있었다. 가족력상 특이 소견은 없었으며 문진 소견상 체중감소, 애성, 호흡곤란, 연하곤란 등의 다른 증상은 호소하지 않았다. 이학적 검사 결과 후두 내시경에서 특이 소견 관찰되지 않았고 갑상선 우측엽 부위에서 4cm 크기의 압통을 동반하는 경부 종물이 촉지되었다. 경부 전산화 단층촬영 결과 석회화를 동반한 저음영의 결절성 병변이 우측 갑상선에서 관찰되었으며 우측 경부 level Ⅲ, Ⅵ에서 괴사성 림프절 소견을 보였다(Fig. 1). 갑상선 결절에 대해서 초음파 유도 하 조직침생검(ultrasound guided core biopsy), 전이성 림프절에 대하여 세침흡인검사를 시행하였으며 병리조직 검사 결과 편평상피세포암과 역형성암종(anaplastic carcinoma) 가능성을 모두 배제할 수 없었다. 전이성 병변 및 이차성 원발암 확인을 위한 검사를 시행하였으며 흉부 전산화단층촬영에서 다수의 전이성 림프절 의심 소견이 관찰되었으나 양전자방출단층촬영(PET-CT)에서는 양성 반응성 림프절(benign reactive lymph nodes)로 확인되었다(Fig. 2).
Fig. 1
Axial CT scan of the neck shows 4 x 4cm sized low density ill defined nodular lesion with calcification in the right thyroid lobe. The mass invades to strap muscle and trachea(A). Axial CT scan of the neck shows enhancing lymph nodes with central necrosis at right Level III(arrow)(B).
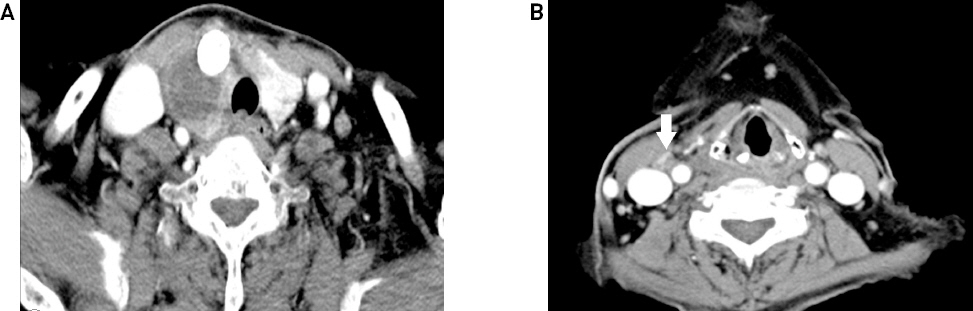
Fig. 2
Chest CT axial view shows multiple lymph nodes enlargement in the mediastinum(white arrow: lower paratracheal node, black arrow: subaortic node)(A). PET-CT axial view shows hyperdense and symmetrical uptake lesions in the mediastinum(B).
내분비내과, 혈액종양내과와 다학제적 회의 후 흉부 전이성 병변에 대한 추가적인 검사 후 수술여부를 결정하기로 하였으나, 환자 및 보호자분 환자 심한 경부 통증에 대한 즉각적인 증상 경감을 원하여 흉부 병변과 상관없이 고식적 갑상선 전절제술과 우측 선택적 경부절제술(selective neck dissection level Ⅲ, Ⅵ) 시행하였으며 기관절개술은 시행하지 않았다. 수술장 소견 상 우측 갑상선 종괴가 피대근, 광경근, 식도, 기관, 피판 등에 육안적 침범 소견을 보였다. 조직검사 결과 절제변연을 침범하는 유두상암종이 혼재된 고분화도의 편평상피세포암 소견을 보였으며 혈관, 림프절, 기관, 주위 근육의 부분적 침범소견을 보였다(Fig. 3). 또한 기관벽, 광경근, 피판 등에도 모두 침범소견 확인되었다. 수술장에서 육안으로 관찰되는 종괴는 모두 절제하였고, 기관벽 유착 부위의 연골을 함께 제거하였다. 되돌이 후두신경 침범 확인되어 종괴와 함께 절제하였다. 면역조직화학염색상 TTF-1, ALK-1은 고분화도의 편평상피세포암에서 음성결과를 보였으나 Thyroglobulin, CK19, CK5/6, High-molecular-weight cytokeratin(CK-HMW)양성결과를 나타내었다(Fig. 4). 또한 분자유전학검사상 ALK gene translocation은 음성으로 확인되었다. 술 후, 술 전 계획한 기관지 초음파 내시경을 이용한 세침흡인술을 시행하였으며 전이성 림프절은 확인되지 않았다.
Fig. 3
Pathological appearance of the tumor. Squamoid cells with cellular pleomorphic and atypical mitosis(H&E, ×200, arrow)(A). Squamous carcinoma with necrosis(H&E, ×200, arrow)(B).
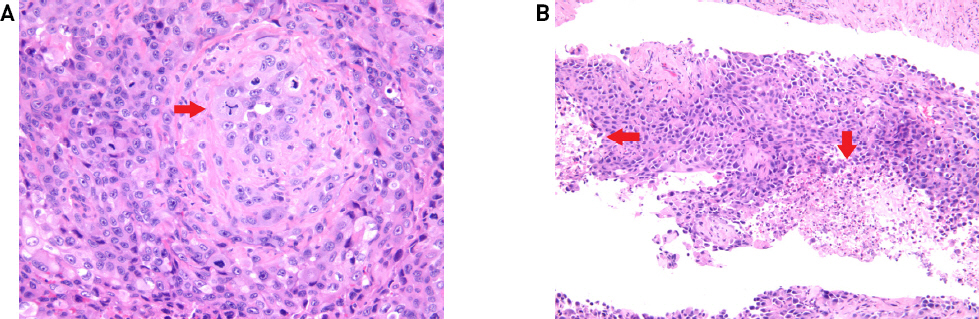
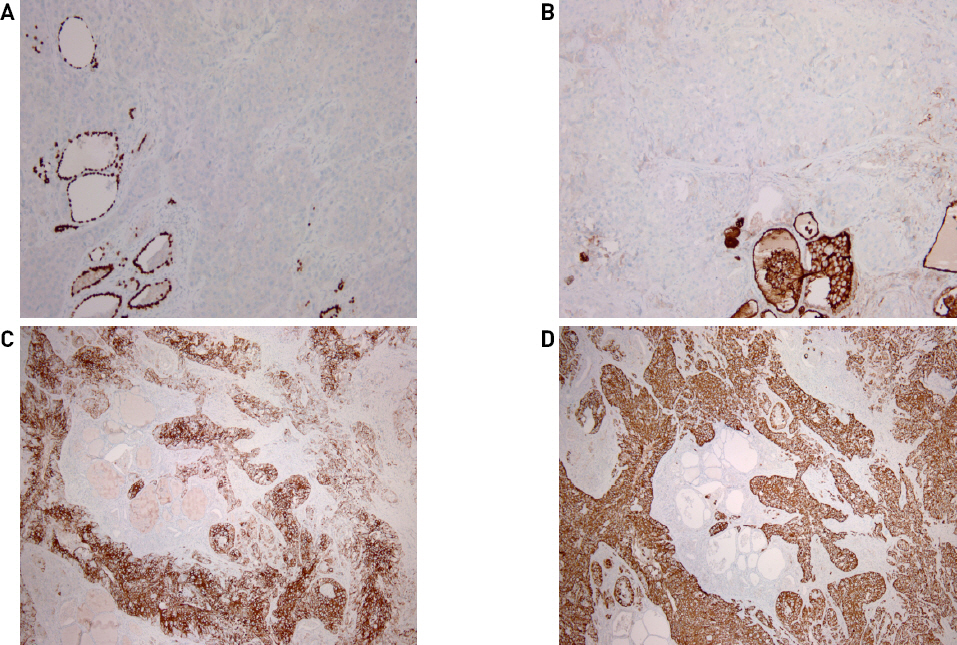
Fig. 4
Immunohistochemical staining results. No immunoreactivity for TTF-1(×100)(A). Focal weak expression for thyroglobulin (×100)(B). Positive staining for CK5/6(×40)(C). Strong immunoreactivity for CK(HMW)(×40)(D).
방사선 종양학과, 혈액종양내과와 협의하여 보조치료요법으로 외부 방사선 조사 및 항암화학요법을 계획하였으나 술 후 14일째, 수술 부위 발적 및 괴사성 경부 병변 있어 경부 전산화 단층촬영, 초음파 유도 세침흡입검사 시행하였다(Fig. 5). 조직검사 결과 역형성 암종이 배제된 편평상피세포암 소견으로 확인되었다. 경부 병변에 대하여 음압생성장치(CURAVAC, Vacuum-Assisted Closure Therapy)에 연결하여 흡인압력을 120mmHg로 유지하였으나 급속한 병변 진행으로 인한 환자의 전신상태 악화 및 구토 시 유발된 흡인으로 보존적 치료를 유지하다 술 후 38일째 흡인성 폐렴으로 사망하였다.

고찰
갑상선에서 발생한 원발성 편평상피세포암은 매우 드문 질환으로 1858년 von Krast가 처음 보고하였으며 전체 갑상선암종의 약 1%를 차지하고 있다.5) 조직학적으로 갑상선은 정상적으로 편평상피가 존재하지 않고 여포세포(follicular cell)와 여포곁세포(parafollicular cell)로 구성되어 있다. 이러한 조직학적 특성으로 인해 갑상선의 원발성 편평세포암종의 발생학적 기원에 대해서는 여러 가지 가설이 제기되어 왔다. 첫째, 갑상선종 등의 비악성 질환에서의 편평상피화생에 의해 발생한다는 설, 둘째, 갑상설관, 흉선, 최종기관지체(ultimobranchial body) 등의 발생학적 잔유물에서 기원한 편평상피세포에서 발생한다는 설, 셋째, 유두상암의 분화에 의해 발생한다는 설 등이 있다.7-11)
일반적으로 원발성 갑상선 편평상피세포암은 성인 여성에서 남성보다 2배 정도 발생률이 높은 것으로 알려져 있고, 주로 50대와 60대에 흔히 발생한다. 갑상선염 혹은 갑상선종의 긴 병력을 가진 환자에서 흔히 발생하며, 갑작스런 종괴의 크기 증가를 경험하는 경우가 많다. 동통, 발열, 연하장애, 애성 등의 증상과 함께 질환은 급속히 진행, 악화되는 경과를 보이며,12) 보고된 몇몇 증례에서와 같이 수술 당시 대부분 주위의 근육이나 식도, 후두, 기도, 주요 혈관 등에 침범된 경우가 많다.1,5)
수술 전 시행하는 세침흡인세포검사, 초음파 검사, 갑상선 기능검사와 스캔, 전산화 단층촬영 및 자기공명영상 등이 진단에 도움이 되나 정확한 진단에는 크게 영향을 미치지 못하는 경우가 많고, 수술을 통한 조직검사로 확진하는 경우가 대부분이다. 원발성 갑상선 편평상피세포암으로 확진하기 위해서는 폐, 두경부, 위장관, 상기도, 신장 등의 원위로부터의 전이를 배제하는 것이 필수적이며 조직병리소견상 각화(keratin) 및 세포간교(intercellular bridge)가 확인되어야 한다.13,14) 또한, 고분화 갑상선 암종, 미분화(역형성) 암종, 수질성 암종, 악성 림프종 등의 질환을 감별할 필요가 있다.
본 증례에서도 술 전 갑상선 우측엽에서 시행한 초음파 유도 하 조직침생검(ultrasound guided core biopsy)에서 편평상피세포암과 역형성암종(anaplastic carcinoma)을 완전히 감별하지 못하여 술 후 조직검사에서 면역조직화학검사를 추가로 시행하였으며 TTF-1, Thyroglobulin음성 및 CK19, CK5/6, High-molecular-weight cytokeratin 양성 소견을 확인하여 편평상피세포암으로 진단하였다. 또한 이차성 편평상피세포암을 배제하기 위해 흉부 전산화단층촬영 및 뇌 자기공명영상, 양전자방출단층촬영(PET-CT) 등의 전신 전이 검사를 시행하였다.
치료 원칙은 예후가 좋지 않아 조기에 발견하여 광범위 외과적 절제를 시행하는 것이 필수적이나 진단 당시 대부분의 경우 주변 조직으로의 침범이 확인되기 때문에 수술 전후 항암 화학요법이나 방사선 치료를 시도해 볼 수 있다.1,5) 5-fluorouracil, bleomycin, vincristine 등의 화학요법이나 방사선 요법의 경우 효과가 거의 없는 것으로 보고 되고 있으나, 최근에 발표된 문헌에서는 술 전후 시행한 화학요법 및 주위 조직 침범이 있는 경우에 외부 방사선 조사가 효과가 있다는 보고가 있다.1,15,16)
본 증례에서도 술 후 화학요법 및 외부 방사선 조사 시행 예정이었으나 환자의 급격한 전신상태 악화로 시행하지 못하여 보조치료요법의 효과에 대한 경과를 얻지는 못하였다.
저자들은 효과적인 치료방법이 아직 확립되지 않은 매우 드문 질환인 갑상선에서 발생한 원발성 편평상피세포암에서, 갑상선 전절제술, 선택적 경부절제술을 시행하였으나 국소 병변 진행으로 술 후 38일 후 사망한 1예를 경험하였기에 문헌고찰과 함께 보고하는 바이다.




