이하선으로 전이된 안검의 피지샘 암종 1예
A Case of Parotid Metastasis from Sebaceous Carcinoma of the Eyelids
Article information
Abstract
= Abstract =
Sebaceous carcinoma is a relatively rare and aggressive malignant tumor. Periocular area (especially eyelid) is the most common lesion to occur, and the most common extraocular lesion is the parotid gland. Because the lesion also mimic other benign inflammatory diseases, this leads to delayed diagnosis or misdiagnosis. Here, we report a 58-year-old male patient who presented with a non-tender painless left parotid mass after wide excision of sebaceous carcinoma in the left eyelid two years ago. When he was diagnosed with sebaceous carcinoma of left eyelid, there was a small left parotid tumor on the computed tomography. But no further examination and treatment were performed. Two years later, physical examination revealed growing parotid tumor and multiple neck nodes on the left side. After radical parotidectomy and neck dissection, histological examination showed a sebaceous carcinoma and neck node metastasis. Considering the aggressiveness of sebaceous carcinoma, further evaluation for parotid glands should be considered when sebaceous carcinoma of the eyelid was discovered. Postoperative chemoradiotherapy was performed for disease control. Follow up after two years, and computed tomography showed no sign of recurrence.
서론
피지샘 암종(sebaceous gland carcinoma)은 피지샘의 부속 상피(adnexal epithelium)에서 발생하는 암으로, 흔하지는 않지만 매우 공격적인 성향을 지니고 있어 전이와 관련된 사망률(metastasis-related mortality)이 높게는 40%까지 보고되기도 한다.1) 피지샘 암종은 눈 주위 영역(periocular region)에 호발하는데 가장 흔하게 발생하는 부위는 안검(eyelid)이며, 두 번째 호발하는 부위는 이하선(parotid gland)으로 알려져 있다.2) 주로 6-70대에서 호발하며, 여성에서 조금 더 많이 발생하는 것으로 알려져 있다. 통증이 없고 천천히 자라는 경우가 많아 임상적으로 양성종양과 큰 차이가 없어 늦게 진단되는 경우도 많다.3) 경부 림프절 전이나 이하선 주변 림프절로 전이가 있을 경우 5년 생존율이 5-60% 정도로 매우 낮아지는 위험한 암종이다.4) 저자들은 안검 종양의 광범위 절제술을 받고 피지샘 암종으로 진단받은 환자에서 수술 당시 관찰되던 이하선 종양이 2년 뒤에 경부 림프절 전이를 동반한 피지샘 암종으로 진단된 1예를 경험하였기에 문헌 고찰과 함께 보고하는 바이다.
증례
기저질환이 없는 58세 남자 환자가 수개월 전부터 점차 커지기 시작한 좌측 이하선의 무통성 종물을 주소로 내원하였다. 신체검사 상 좌측 이하선 부위에 약 2 x 3 cm 크기의 단단하고 주변 조직과 고정된 양상의 종물이 촉진되었다. 좌측 경부 level II에는 1 x 1 cm 가량의 림프절 비대가 관찰되었고 안면마비는 관찰되지 않았다. 환자는 2년 전 좌측 하안검 부위에 생긴 종물로 본원 안과에 내원한 과거력이 있었다. 당시 시행한 안와 컴퓨터 단층 촬영 검사(orbital CT)에서 1.1 x 0.9 cm 크기의 비균질성의 조영 증강을 보이는 결절성 병변이 좌측 하안검 부위에 관찰되었으며, 원뿔 내외 공간(extra & intraconal space)으로의 침범은 보이지 않았다(Fig. 1A). 안검 종물과 함께 좌측 이하선에 1cm 가량의 약하게 조영 증강되는 종물이 관찰되고 있으나, 당시에는 이하선 종양에 대한 추가 검사는 진행되지 않았다(Fig. 1B). 본원 안과에서 하안검 종물에 대해서 국소마취하에 절제 생검술(excisional biopsy)을 시행하였으며, 조직병리학적 검사 상 미분화된 양상의 악성 종양이 의심되는 결과가 보고되어 추가 수술이 필요한 상황이었다. 이후 환자는 연고지 관계상 타 병원에 내원하여 국소마취하에 외안각(lateral canthus)을 포함한 하안검 가측 일부에 대해 추가적인 광범위 절제술을 시행 받았으며 최종 조직병리 검사 상 최장 길이는 0.7 cm, 두께는 0.4 cm인 피지샘 암종으로 확인되었다. 5 mm 이상의 절제연을 확보하였고, 신경 주위 침윤(perineural invasion), 림프 혈관 침윤(lymphovascular invasion)은 관찰되지 않았다. 이후 환자는 추가 치료 없이 수술을 시행 받은 병원에서 추적 관찰을 하였다.
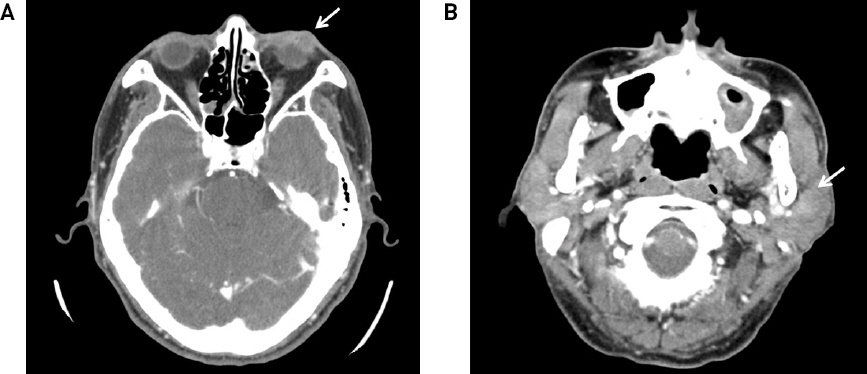
Preoperative imaging evaluation of the eyelid mass. (A) Enhanced CT scan showed heterogeneous mass in the left lower eyelid (white arrow). (B) A small mass of the left parotid gland was incidentally observed at the time of diagnosis (white arrow).
환자는 안검 종양을 수술한 지 2년이 지나 이하선의 종물을 주소로 본원 외래에 내원하였다. 내원 당일 종물의 정확한 조직학적 평가를 위해 세침 흡인 세포 검사를 시행하였으며, 병리과로부터 선낭 암종(adenoid cystic carcinoma) 혹은 전이성 암종(metastatic carcinoma)이 의심된다는 소견을 받았다. 종양의 분화가 좋지 않아 세침 흡인 검사만으로는 정확하게 평가가 어려워 이하선 종물에 대한 병리학적 확진을 위하여 수술적 제거를 계획하였다. 수술 전 시행한 경부 컴퓨터 단층 촬영 검사(neck CT)에서는 약 3 x 2.2 cm 크기의 주변과 경계가 명확하지 않으며 조영이 증강되는 타원형의 종물이 좌측 이하선 천엽에서 기시하여 심엽까지 일부 확장되어 있는 것을 관찰할 수 있었다(Fig. 2A). 또한, 좌측 경부 level II 구역에도 전이를 의심할만한 림프절들이 관찰되었다(Fig. 2B, 2C). 양전자 방출 단층 촬영 검사(PET-CT)에서는 표준화 섭취 계수(standard uptake value, SUV) 8.6의 고대사(hypermetabolic) 종물이 좌측 이하선에서 관찰되었으며(Fig, 2D), level II, III의 경부 림프절도 전이가 의심되는 상황이었다(Fig. 2E, 2F). 타 장기로의 원격 전이는 관찰되지 않았다(Fig. 2G). 침샘암 및 경부 림프절 전이 의심 하에 이하선 전절제술 및 제2형 변형 근치적 경부 절제술을 시행하였다(Fig. 3). 수술 당시 이하선 종물은 안면신경의 기시부와는 분리가 되었으나, 저작근과 안면신경의 가지에 유착되어 있어 경부 가지(cervical branch)와 변연 하악 가지(marginal mandible branch)를 제외한 안면신경의 분지들은 희생되었다. 이하선의 심엽은 이복근(digastric muscle), 경상 설골근(stylohyoid muscle), 그리고 경상돌기(styloid process)로부터 박리하여 분리시켜 제거하였다. 전반적으로 종물이 주변의 근육과 유착되어 있어 근육을 일부 포함하여 적절한 변연을 확보하며 종물을 제거하였다. 수술 후 10일째 배액관 제거 후 특이 합병증 없이 퇴원하였다. 제거된 이하선 종양은 3.2 x 3.0 x 1.7 cm의 크기로 최종 조직병리소견 상 H&E 염색에서 거품 세포질(foamy cytoplasm) 양상의 공포성 세포질(vacuolated cytoplasm)을 가진 세포가 기저양 세포(basaloid cell)로 둘러싸인 모습이 보이며 세포 간의 경계가 불분명하게 관찰되었다. 또한 표피층까지의 파제트병 모양의 성장(pagetoid growth)이 보이며 주위로 괴사 소견이 관찰되었다(Fig. 4A, 4B). 면역조직화학검사 상 피지 세포에서 특징적으로 양성반응을 보이는 epithelial membrane antigen (EMA), androgen receptor (AR) 염색에서 양성반응을 보여 최종적으로 피지샘 암종으로 진단하였다(Fig. 4C, 4D). 상기 이하선 암종은 절제연이 양성이었으며, 고분화성 종양으로 샘외 침범(extraglandular extension)이 관찰되었고 신경 주위 침윤, 림프 혈관 침윤이 모두 관찰되었다. 경부 림프절 조직은 8개에서 전이성 암종이 확인되었으며, level II의 4개의 림프절에서 피막외 침범(extranodal extension)이 확인되었다. 환자의 병리 결과를 종합하여 pT2N2bM0로 AJCC 병기 IVA로 최종 진단하였다. 수술 후 다학제 진료를 통해 시스플라틴을 기반으로 한 동시 항암방사선치료를 진행하였다. 6차례에 걸쳐 항암제를 투여하였고, 33회에 걸쳐 좌측 경부 림프절 부위에 61.05Gy, 이하선 부위에 69.96Gy의 방사선치료를 시행하였다. 환자는 항암방사선치료 종료 후 2년까지 영상학적 검사에서 재발 소견은 관찰되지 않고 있다. 안면 마비는 House-Brackmann grade 5 수준으로 관찰되어 보존적인 치료를 유지하고 있으며, 외래에서 재발 여부를 지속적으로 추적 관찰할 예정이다.
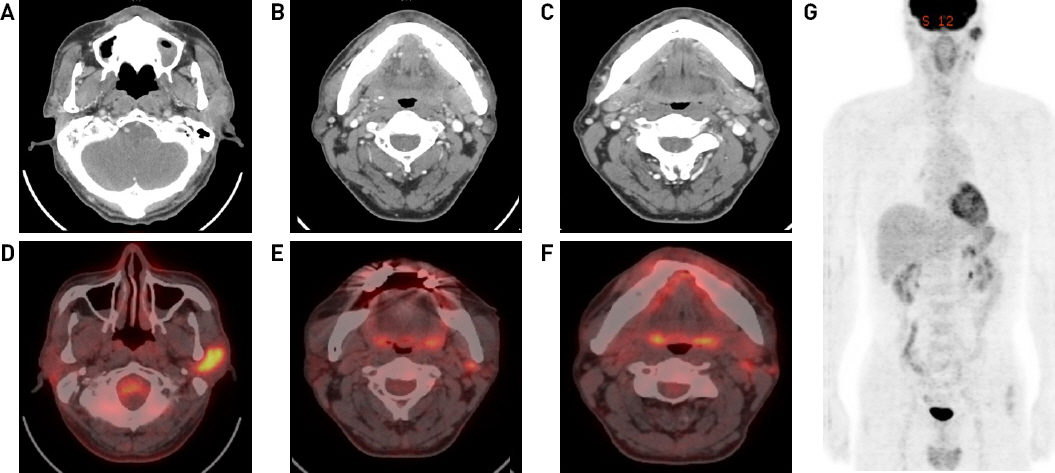
Preoperative imaging studies. (A-C) Enhanced CT scan showed a 3.0 x 1.6 x 2.2 cm sized ill-defined lobulated mass in the left parotid gland and multiple enlarged lymph nodes. (D-G) Axial fused image of PET-CT scan showed intense FDG uptakes at the left parotid gland and level II lymph nodes. No distant metastases were revealed.
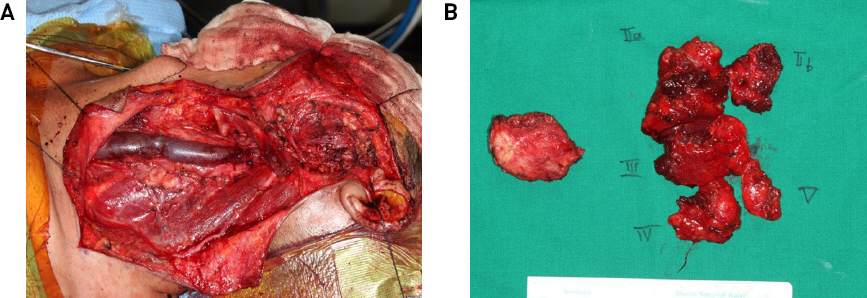
Intraoperative findings and resected specimens. (A) Image shows the surgical site after left radical parotidectomy and neck dissection. (B) 3.2 x 3.0 x 1.7 cm sized firm, irregular surfaced parotid gland mass and left level II-V lymph nodes.

Microscopic and immunohistochemistry findings. (A) H&E staining shows the tumor lobules composed of large foamy cells surrounded by basaloid cells (x 200). (B) Numerous cells with sebaceous differentiation is shown (x 200). (C) Diffuse positive for epithelial membrane antigen (EMA) is shown (x200). (D) Diffuse positive for androgen receptor (AR) is shown (x200).
고찰
피지샘 암종은 1-5% 가량의 빈도로 발생하는 비교적 드문 악성 종양으로, 안검에 생기는 악성 종양 중 기저 세포암(basal cell carcinoma)과 편평 세포암(squamous cell carcinoma)에 이어 3번째로 많이 발생하는 것으로 알려져 있다.5) 피지샘 암종은 초기에는 임상적으로 안검 결막염 같은 염증성 질환과 유사하게 보이는 경우가 많아 진단이 늦어지는 경우가 많다.6,7) 노령, 여성, 아시아인, 두경부 영역에 방사선 치료를 받은 과거력, Muir-Torre syndrome의 유전적 소인, 가족성 망막모세포종(familial retinoblastoma) 등이 현재까지 알려진 발병의 위험인자이다.8-11) 피지샘 암종은 세포 이형성 정도에 따라 고분화(well-differentiated), 중분화(moderate-differentiated), 저분화(poorly-differentiated)로 분류하긴 하지만, 조직학적으로도 다양한 표현형을 지니기 때문에 병리 진단이 쉽지 않다. 세포형태학적으로 피지샘 암종은 표피층으로의 파제트병 모양 전파(pagetoid spread)를 동반한 소엽상 성장(lobular growth)과 공포성 세포질(vacuolated cytoplasm)이 정중앙에 위치한 다각형의 세포(polygonal cell)들이 군집을 이루거나 산재한 형태로 나타난다.12) 현미경적으로는 다공포성의 투명 세포질(multivacuolated clear cytoplasm)을 동반한 세포 소엽(cell lobule)이 관찰되며, 핵-세포질 비(nucleo-cytoplasmic ratio)가 증가하고, 응집된 염색질이 나타난다.13) 면역조직화학 염색에서는 종양 세포에서 피지(sebaceous) 혹은 선상(glandular) 분화가 동시에 확인되기도 한다.14) 또한, EMA, AR, anti-epithelial antigen (BerEP4), anti-adipophilin (ADP), p53, Ki-67등의 면역조직화학 염색을 통해 편평 세포암이나 기저 세포암과 감별할 수 있다. 감별진단이 필요한 기저 세포암의 경우 EMA에서 음성반응을 보이며, 편평 세포암의 경우 AR에서 음성반응을 보이게 된다.15)
피지샘 암종의 치료는 5mm 이상의 충분한 절제연을 확보하는 수술적 절제가 원칙이다. 국소 림프절 전이가 있을 경우에는 원발 부위의 절제와 경부 림프절 절제술을 함께 시행하며, 수술 후 방사선 치료를 권고하고 있다.6,16,17) 일반적으로 피지샘 암종의 경우 신경 주위 침윤이 약 20% 정도에서 관찰되나 림프 혈관 침윤은 드문 것으로 알려져 있는데, 본 환자의 경우 신경 주위 침윤과 림프 혈관 침윤이 모두 관찰 되었다. 일반적으로 피지샘 암종의 치료에 항암치료를 적용하지 않고 있으나, Jung 등은 재발한 전이성 피지샘 암종 환자에서 5-플루오로우라실과 시스플라틴의 병합 요법을 이용하여 치료한 사례를 보고한 바가 있다.18) 수술 후 동시 항암방사선치료가 방사선치료 단독에 비해 생존율에 이익을 주는 지에 대한 연구는 아직까지 부족하다. 하지만 본 증례의 경우 환자의 전신 상태가 양호하였고 치료에 적극적이었으며, 이하선 종양의 조직학적 소견을 고려하여 의료진의 상의 하에 동시 함암방사선치료를 하기로 결정하였다. 수술 후 동시 항암방사선치료의 효과를 증명하기 위해서는 많은 수의 환자를 대상으로 추가 연구가 필요할 것으로 생각된다.
본 증례의 경우 타 병원에서 수술 당시 안검 종물의 평가를 위해 시행한 안와 컴퓨터 단층 촬영 검사에서 안검 종물과 함께 좌측 이하선에 1cm 가량의 약하게 조영 증강되는 종물이 관찰되었다(Fig. 1B). 2년 후에 동일한 좌측 이하선 부위에 발생한 피지샘 암종은 안검의 원발 병소와 병리학적으로 동일하다는 점과 암종이 발생한 시기의 시간적 선후관계를 고려하였을 때, 안검의 피지샘 암종이 발견되었을 당시에도 전이의 가능성에 대한 충분한 평가가 필요하였을 것으로 생각된다. 피지샘 암종의 공격성을 고려하였을 때 이하선 종물에 대한 적극적인 치료가 고려되어야 했으나 원발 부위만 치료하고 종료하였던 점이 다소 아쉬운 부분으로 생각된다. 피지샘 암종의 경우 인종별로 임상 양상 및 전이 패턴이 다소 차이가 있으며, 종양 자체가 흔하지 않기 때문에 전이에 대한 진단 및 치료가 늦어지는 경우가 있을 수 있다. Park 등이 29명의 한국인을 대상으로 눈 주위에서 발생한 피지샘 암종 환자들의 임상병리학적 분석 결과를 보고한 논문에서도 1명에서만 경부 전이가 확인되었다.19) 이와 같이 한국인의 경우 피지샘 암종의 전이 양상이 기존에 서양인에서 보고된 바와 다소 차이를 보이고 있기 때문에 안검 주위의 악성 종양으로 진단된 환자에서 이하선 및 주위 림프절 영역에 대해 전이를 간과할 가능성이 있을 수 있다. 저자들은 상기 증례를 통해 안검에 발생한 악성 종양의 경우에 두경부 영역으로의 전이 여부를 보다 적극적으로 평가할 필요가 있다는 것을 확인하였다. 추후 피지샘 암종의 국소 전이에 대한 정확한 진단과 치료 지침을 제시하기 위해서는 더 많은 증례 분석이 필요할 것으로 생각된다.